Please provide either your email id or phone through which we can contact back. Your information will remain confidential with IGES. We will try to respond promptly.
The YP Foundation conducted youth-led audits of healthcare services in partnership with Asian Bridge India in Varanasi and Action India in North East Delhi. 30 youth leaders audited 63 health facilities on youth friendliness and co-created these comic strips and posters along with recommendations for multiple stakeholders through the Audit Report.
The dominant discourse and context in India, in which contraceptives have been located, promoted, and disseminated has been that of population control and family planning. Consequently, it has overlooked a whole gamut of issues as well as the needs of large groups of populations who have been denied relevant access and information. They include: the pursuit of sex for pleasure beyond procreation; the needs of young and unmarried persons; the unique contraceptive needs of trans and non-binary persons; sexual and reproductive health issues of persons with disabilities; the issues of access and gender discrimination; and contraceptives as a way to protect against sexually transmitted infections. One of the core influencers of the ecosystem determining information, access, and design is the policy of the government and the programmes that flow from it. To change the reality of contraception and ensure it meets the needs of all, there is an urgent need to advocate with the government to change its approach and policy.
In collaboration with UNFPA, TYPF has created Handbooks for ASHA workers and other Front Line Service Providers to understand and practice youth friendliness while providing counselling or other services to youth and adolescents. TYPF is committed to ensuring that young people have affirming and happy experiences when seeking sexual and reproductive health information, services and products. A key aspect of this work is to create resources and work with service providers who work with young people to improve their perspective, practices and skills to engage more sensitively with youth and adolescents. This kit is a part of this commitment and work. It includes training manuals for those who want to work with ASHAs or other service providers to enhance their service quality as well as handbooks that can be used by the service providers themselves. These are made in collaboration with the UNFPA India office and we acknowledge their support, partnership and guidance in this work.
In 2002, commercial surrogacy was legalized in India. Over the next decade, the industry grew tremendously, estimated to be a $2 billion a year business. However, a number of incidents between 2002 and 2015 highlight the absolute disregard for the rights of the surrogate mother and child, the lack of comprehensive laws related to surrogacy, and the exploitation of loopholes within the already existent ones.
Consider the case of Baby Manji Yamada in 2008. In 2007, a doctor working at an infertility clinic in Gujarat, arranged for a Japanese couple to have a child through surrogacy. The surrogate mother was impregnated using a mix of the father’s sperm and an anonymous Indian woman’s egg. However during the course of the pregnancy, the couple filed for divorce, and there were no laws in place which covered whose child the baby would be; the women who donated the egg or the surrogate mother or the father. In the wake of this, a petition was also filed against the doctor stating that he was running a child trafficking racket by taking advantage and making money off the lack of surrogacy laws. The case of Baby Manji was resolved when her grandmother took her in, but by then the question of the ethical violations of the booming surrogacy industry had already entered the public arena.
In another instance, in 2012 an Australian couple had twins by surrogacy, but took only one home rejected the other. Then there was the case of a single mother from Chennai who opted to becoming a surrogate in the hopes of using the payment to start a shop of her own; however, she received minimal financial remuneration as the autowallah who acted as the middleman took 50% of the cut. In 2014, a 26-year-old woman died after complications from a surgical procedure to harvest eggs from her body, as part of an egg donation programme at a private clinic in New Delhi.
In addition to the series of PILs that emerged which sought to ban commercial surrogacy, the 228th report of the Law Commission recommended prohibiting commercial surrogacy and allowing altruistic surrogacy. The exploitation of women who became surrogates due to a paucity of employment options, and the easy abandonment of the children born under these situations led to the Union Cabinet approving the Surrogacy (Regulation) Bill of 2016, which effectively banned all forms of commercial surrogacy. Altruistic surrogacy refers to an arrangement between a couple and a surrogate without any transfer of funds, except for the payment of medical expenses. Altruistic surrogacy is practiced in some centres in India, but a majority of centres are primarily for commercial surrogacy.
Though the intent of the bill was to curb the exploitation of women, there seems to be more wrong with it than right. It shows a shallow understanding of how to deal effectively with issues, where outright prohibition is chosen as a solution, as opposed to delving deeper into the intricacies of the problem and instituting issue-specific policies and regulation. The medical community, and even some factions of the general public have criticized the bill for being discriminatory and draconian even while it has been understood as necessary in curbing the ‘baby-making industry’. The health minister has said that the bill is open to improvements, but the clauses detailing the exploitation of the surrogate mother and child will not be compromised on.
While the bill bans commercial surrogacy and institutes heavy penalties and jail time for establishments found indulging in it, it also heavily regulates the conditions that a couple must fulfill to be able to opt for surrogacy. The couple must have been married for a minimum of 5 years, and at least one of them proven infertile. The couple must have Indian citizenship, with the female aged between 23 and 50, and the male between 26 and 55 years. Due to these strict conditions, homosexual couples, single parents, unmarried couples and couples with children (biological, adopted or surrogate) do not qualify for surrogacy under the new bill.
The bill also heavily regulates the role of the surrogate. For a women to be a surrogate she must be an ‘altruistic relative’ which means she must be a close relative of the couple and must be between 25 and 35 years of age. She can also act as a surrogate only once in her lifetime. The child born through surrogacy will have all the rights of a biological child.
There has been extensive debate on the stringent criteria the couple and surrogate mother must meet in order to go through with the surrogacy. The necessity of the surrogate being a relative and then being a surrogate only once severely limits the options the couple has, with adoption being the only other alternative. A reason given for these strict conditions has been for the promotion of adoption, but that itself comes with a whole slew of problems. Adoption regulations are themselves equally stringent (again, excluding single men, and various other kinds of atypical family set-ups), and processes are hardly streamlined, among other issues. Adoption, then, is hardly a plausible alternative.
Another point of contention is the issue of the surrogate’s consent. After the boom in the industry post-2002, surrogacy came to be stable source of income for many women. If a woman willingly consents to being a surrogate, is assured of a safe medical environment and the child is assured of a safe home, then why should commercial surrogacy be banned outright? Of course, exploitation is a continuing threat and a legitimate issue, akin to the threat of exploitation in the case of sex work. But, like sex work is recognised, regulated in many countries and sex workers given full constitutional rights, surrogacy laws should be put in place to regulate policies and not to institute a blanket ban. Laws need to be implemented in a way that the rights, livelihoods, and decision-making power of those most vulnerable are protected.
One of the most criticized aspects of the bill is the prohibition of anyone other than a heterosexual married couple opting for surrogacy. To exclude single parents, or couples who do not fit a hetero-normative mold, furthers a patriarchal understanding of what constitutes the ‘ideal’ family, and, in other ways, further embeds homophobia into our legal system.
We need to accept that these issues are never black or white, nor can they ever be, and that it’s about time we learn how to navigate this grey expanse. It is hard to paint commercial surrogacy as ‘evil’ or ‘bad’ when it does benefit some people and is often the sole option available for both couples and surrogates. Similarly, altruistic surrogacy at its core is non-exploitative but still proves to be extremely restrictive. Some key points to keep in mind are the benefits of restructuring versus outright banning, and the question of consent versus exploitation. If one if able to assess these issues pragmatically, then the solutions that are offered may truly have positive on-ground impact.
In Safe Hands: A Resource Guide Towards Inclusive Healthcare
This handbook is intended to guide healthcare professionals in providing rights-affirming access to health services to LGBTQIA+ young people. There is enough evidence and lived narratives of persons from the LGBTQIA+ community that shows how they often experience higher rates of health disparities. Their experiences of seeking health services are tenuous and fraught with the possibilities of discrimination and violence.
Centered around building a comprehensive approach to close the gap between the service provider and queer-trans* service seekers, this handbook illustrates the unique concerns, vulnerabilities, and needs of queer-trans* youth when it comes to access to healthcare services. It also helps healthcare professionals comprehend different terminologies and answers FAQs relevant to queer-trans* identities. As a conclusion, the handbook also outlines some possible and tangible recommendations that can be inculcated in healthcare practice and institutions.
Seen Not Heard: Youth-Led Audit of Sexual and Reproductive Health Services in Lucknow
While as a country we continue to highlight the large numbers of young people and claim to make investments in them as the future of the nation, there are few attempts to include young people’s voices in policies and programmes that address their health. This youth led audit of health services in Lucknow highlights this very gap in sexual and reproductive health service provision for young people. The research report presents insights into young people’s experiences of accessing health care and youth friendliness of existing services.
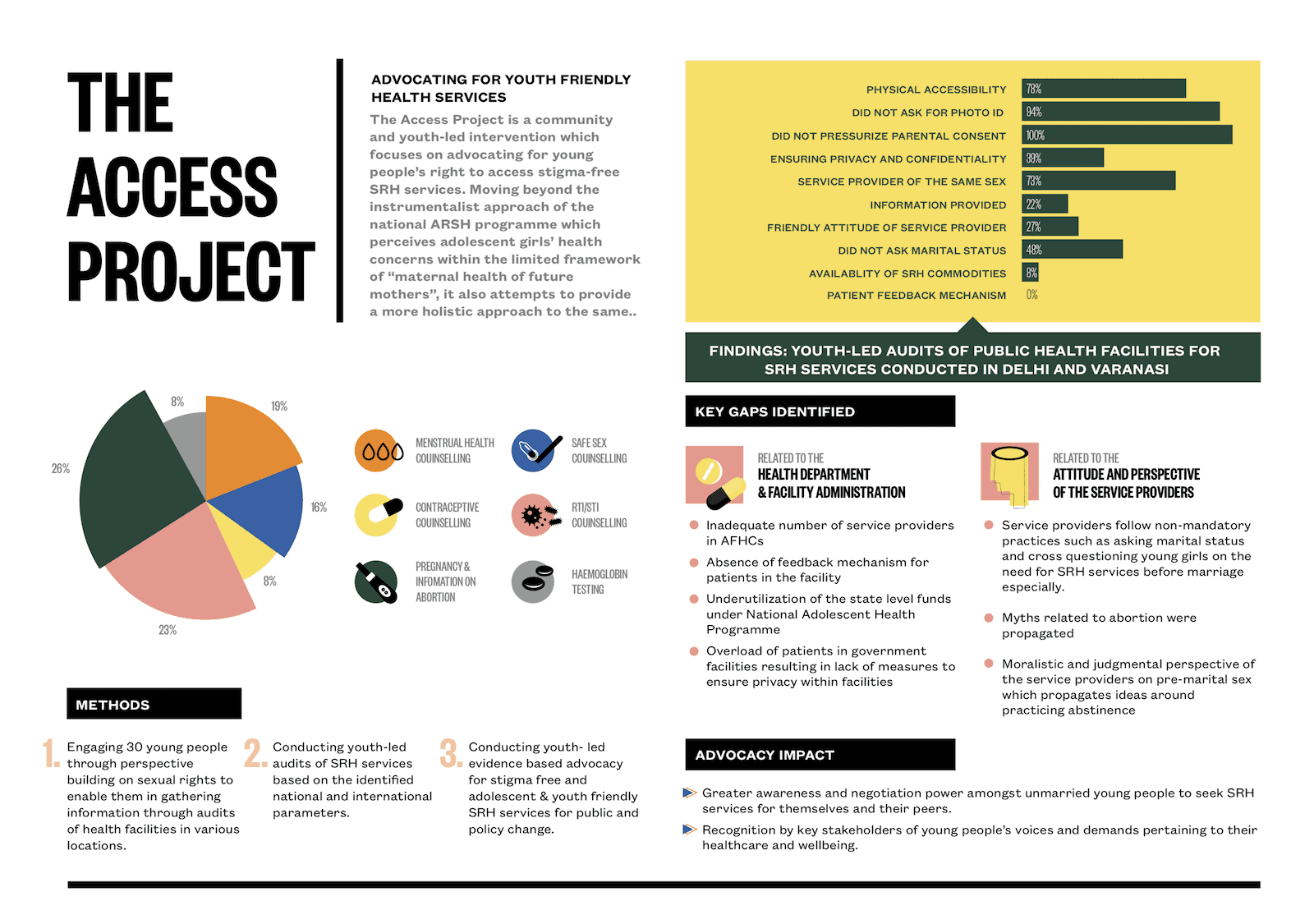
Audit Report and Study Design – The Access Project
Building off the findings of Seen, Not Heard, The Access Project expanded the audit of health services to two districts in Delhi and one district in Varanasi, with the support of two partner organisations in Uttar Pradesh. This report documents the findings of the audit, as well as the process of training researchers and developing a prototype of youth-led research on access to health services. As a conclusion, the report outlines our policy asks, directed towards policy makers, health system officials, front line health workers, and researchers working at the intersection of human rights and youth rights.
Mardon Wali Baatein: A Research Project on Men, Masculinities and SRHR
With the hope of informing SRHR programming for men, both organisationally and within the sector, this exploratory research project asks how masculinities are constituted and expressed by young college-going men in urban Uttar Pradesh. Conducted across three locations with 80 young men (18-26 years old), this qualitative research explores the intersections between gender, sexuality, caste, class, and religion in discussions on masculinities, with a specific focus on sexual health, contraception, and violence. Mardon Wali Baatein further explores the impact of social media and technology on masculinity.